The Digital Education Lab: Your key to peer insights on KESIMPTA
Tap into the RMS experts and unlock the answers to your questions on KESIMPTA
This information is intended for US health care professionals only.
This information is intended for US health care professionals only.
Get fresh perspectives on the 7-year data release for KESIMPTA as 2 RMS experts provide their insights on a growing body of evidence for its use in RMS.
Dr Hauser did not receive compensation for contributing to this material.
Copy Link
Like
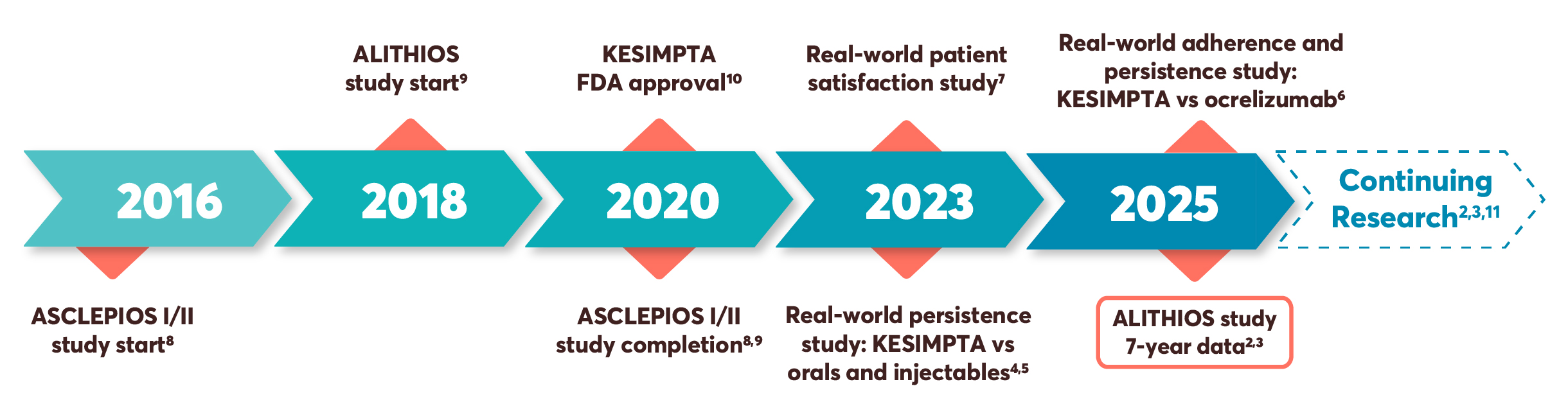
The Body of Evidence for KESIMPTA in RMS Is Continuously Growing1,2
KESIMPTA aims to address the needs of both HCPs and patients with an ongoing evaluation of its long-term efficacy and safety. Backed by pivotal trials, KESIMPTA also provides evidence from real-world studies and up to 7 years of data from the ALITHIOS extension study.1—7
I was very optimistic when ASCLEPIOS trial data were released that we had a therapeutic agent that is effective* with a well-established safety profile. To now see the results from the 6- and now 7-year data is promising.1—3,8,10,12
—Stephen L. Hauser, MD
Dr Hauser was not compensated for this insight.
*As evidenced by reduction in ARR, MRI (Gd+ T1 and T2 lesions), and 3- and 6-month CDP vs teriflunomide. Primary end point: ARR 51% (0.11 vs 0.22), 58% (0.10 vs 0.25). Secondary end points: reduction of number of Gd+ T1 lesions per scan, 98% (0.01 vs 0.46), 94% (0.03 vs 0.52); reduction of annualized rate of NE T2 lesions, 82% (0.72 vs 4.00), 85% (0.64 vs 4.16); 3-month CDP risk reduction 34% (10.9% vs 15.0%); 6-month CDP risk reduction 32% (8.1% vs 12.0%).1,8
FDA, Food and Drug Administration; HCP, health care professional; RMS, relapsing multiple sclerosis.
KESIMPTA Has Powerful Efficacy and Its Self-Administration Can Help Give a Sense of Control for Patients With RMS1
I welcomed the ability to offer patients an option that doesn’t involve traveling to an infusion center—all while having an established efficacy and safety profile.1*
—Amy Perrin Ross, APN, MSN, CNRN, MSCN
The perspectives provided within this newsletter by Ms Ross are her own and not reflective of her affiliation. She has been compensated by Novartis Pharmaceuticals Corporation to provide her perspective.
KESIMPTA is the first and only at-home, self-administered B-cell therapy for RMS, showing demonstrated efficacy* and a proven safety and tolerability profile. The self-administration of KESIMPTA can provide patients with a sense of control over their treatment administration.
*As evidenced by reduction in ARR, MRI (Gd+ T1 and T2 lesions), and 3- and 6-month CDP vs teriflunomide. Primary end point: ARR 51% (0.11 vs 0.22), 58% (0.10 vs 0.25). Secondary end points: reduction of number of Gd+ T1 lesions per scan, 98% (0.01 vs 0.46), 94% (0.03 vs 0.52); reduction of annualized rate of NE T2 lesions, 82% (0.72 vs 4.00), 85% (0.64 vs 4.16); 3-month CDP risk reduction 34% (10.9% vs 15.0%); 6-month CDP risk reduction 32% (8.1% vs 12.0%).1,8
Superior ARR reductions of 51% (0.11 vs 0.22), 58% (0.10 vs 0.25) vs teriflunomide
Relative reduction in mean number of Gd+ T1 lesions per MRI scan vs teriflunomide of 98% (0.01 vs 0.46), 94% (0.03 vs 0.52)
Relative reduction in NE T2 lesions per year vs teriflunomide of 82% (0.72 vs 4.00), 85% (0.64 vs 4.16)
Reduced risk of CDP at 3 months in a pooled analysis vs teriflunomide of 34% (10.9% vs 15.0%)†
†Disability progression was defined as an increase in EDSS of at least 1.5, 1, or 0.5 points in patients with a baseline EDSS of 0, 1 to 5, or 5.5 or greater, respectively. Proportion of patients with 3- or 6-month CDP refers to Kaplan-Meier estimates at month 24.1
ASCLEPIOS I & II study design: ASCLEPIOS I and II were 2 identical, randomized, active-controlled, double-blind, Phase 3 studies in patients with RMS, approximately 40% of whom were DMT treatment naïve. Patients were randomized to double-dummy subcutaneous KESIMPTA (20 mg every 4 weeks) or oral teriflunomide (14 mg daily) for up to 30 months. The primary end point was ARR. Key secondary end points were number of Gd+ T1 lesions and annualized rate of NE T2 lesions and reduction in risk of 3-month CDP. Treatment duration was variable based on end-of-study criteria. Maximum duration 120 weeks, median duration 85 weeks.1
KESIMPTA offers an established safety profile comparable to teriflunomide, an oral therapy1
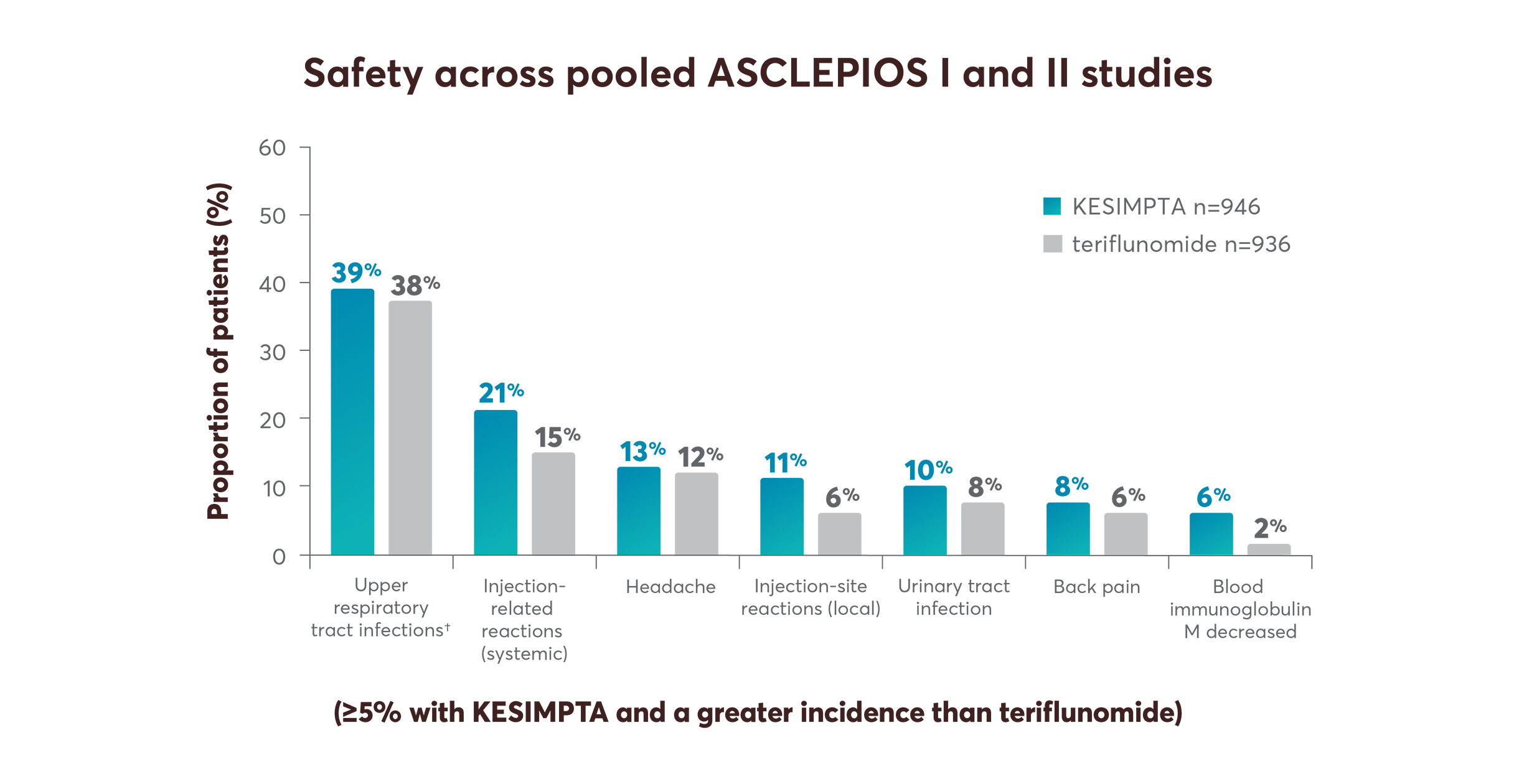
The overall rate of infections and serious infections in patients treated with KESIMPTA was similar to Aubagio (51.6% vs 52.7%, and 2.5% vs 1.8%, respectively).1
ARR, annualized relapse rate; CDP, confirmed disability progression; DMT, disease-modifying therapy; EDSS, Expanded Disability Status Scale; Gd+, gadolinium-enhancing; IRR, injection-related reaction; MRI, magnetic resonance imaging; NE, new or enlarging; RMS, relapsing multiple sclerosis.
†Includes the following: nasopharyngitis, upper respiratory tract infection, influenza, sinusitis, pharyngitis, rhinitis, viral upper respiratory infection, tonsillitis, acute sinusitis, pharyngotonsillitis, laryngitis, pharyngitis streptococcal, viral rhinitis, sinusitis bacterial, tonsillitis bacterial, viral pharyngitis, viral tonsillitis, chronic sinusitis, nasal herpes, tracheitis.
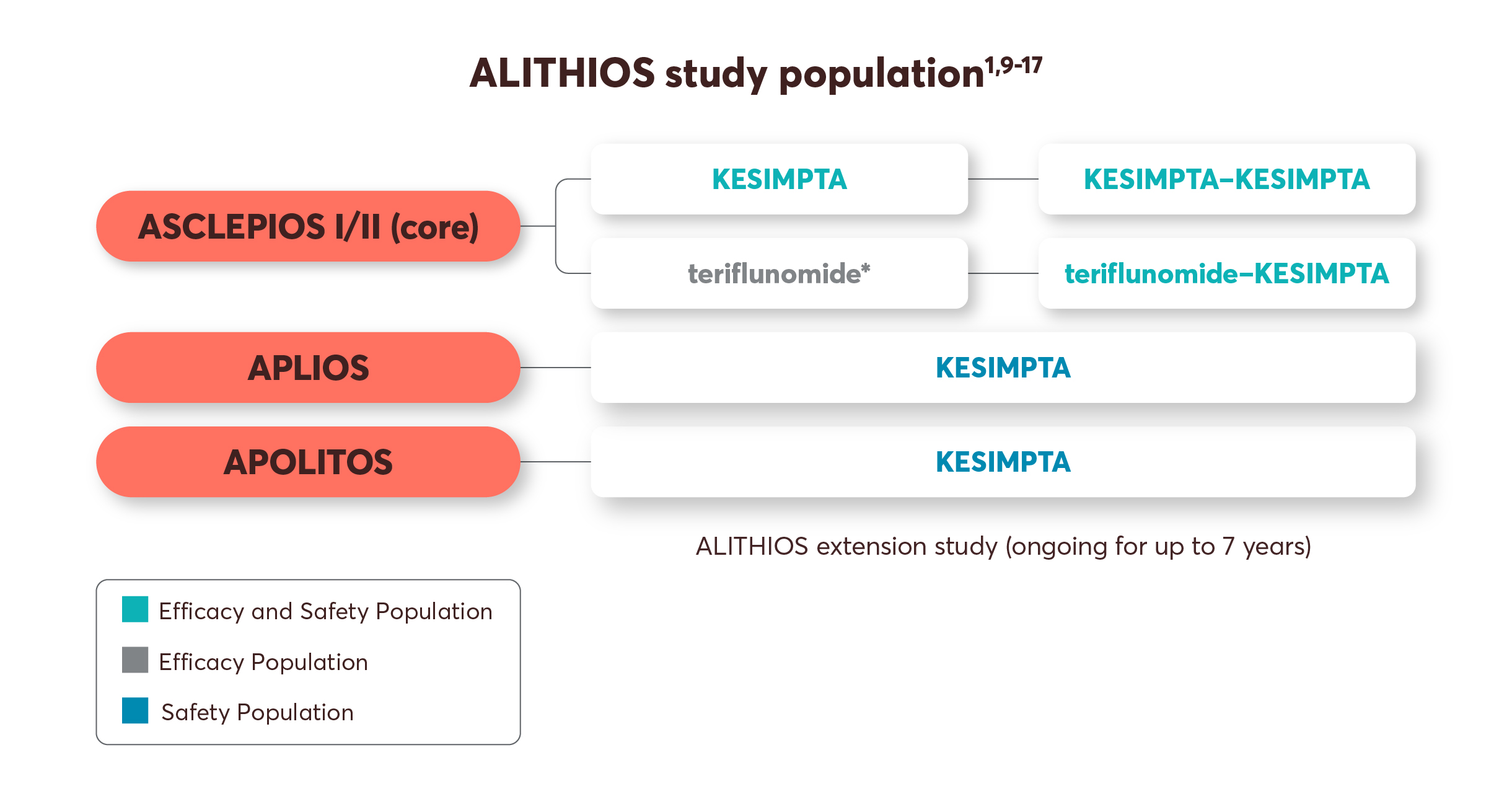
ALITHIOS Study Prioritized Safety As the Primary Objective2,11
With up to 7 years of data, ALITHIOS continues to assess the safety and efficacy of KESIMPTA in patients with RMS from the ASCLEPIOS I/II, APLIOS, and APOLITOS trials.2
With RMS, patients will likely require long-term treatment. So, they are naturally looking to hear about long-term evidence. I feel more prepared for these conversations now that I can share the data from ALITHIOS that show up to 7 years of outcomes.2,10
—Stephen L. Hauser, MD
ALITHIOS study design: ALITHIOS is an open-label, umbrella-extension, Phase 3b, single-arm study evaluating long-term (up to 7 years) data. The primary objective is to assess safety and tolerability (N=1969) in patients with RMS who had at least 1 dose of KESIMPTA (20 mg SC) (including dropouts) from the ASCLEPIOS I/II, APLIOS, and APOLITOS trials. APLIOS (N=284) was a Phase 2, 12-week, open-label, parallel-group study. APOLITOS (N=62) is a Phase 2, 24-week, double-blind, placebo-controlled, parallel-group core-part followed by an open-label extension–part for up to 48 weeks study in Japan and Russia. The secondary objective was to assess efficacy (N=1367) in patients with RMS who had at least 1 dose of KESIMPTA (20 mg SC) from the ASCLEPIOS I and II trials who continued or switched on to KESIMPTA treatment. Long-term (up to 7 years) analysis (n=465) was conducted to evaluate efficacy in the recently diagnosed treatment-naïve subgroup treated with KESIMPTA.2,3,9,11,13,14
Limitations: This analysis represents chance findings. The open-label extension study was not blinded, not controlled, and included inherent self-selection bias for remaining in the trial. This study is an ongoing trial and the data presented are an interim analysis.
No conclusions of statistical or clinical outcomes can be drawn.
RMS, relapsing multiple sclerosis; SC, subcutaneous.
*Control arm in ASCLEPIOS I/II.1
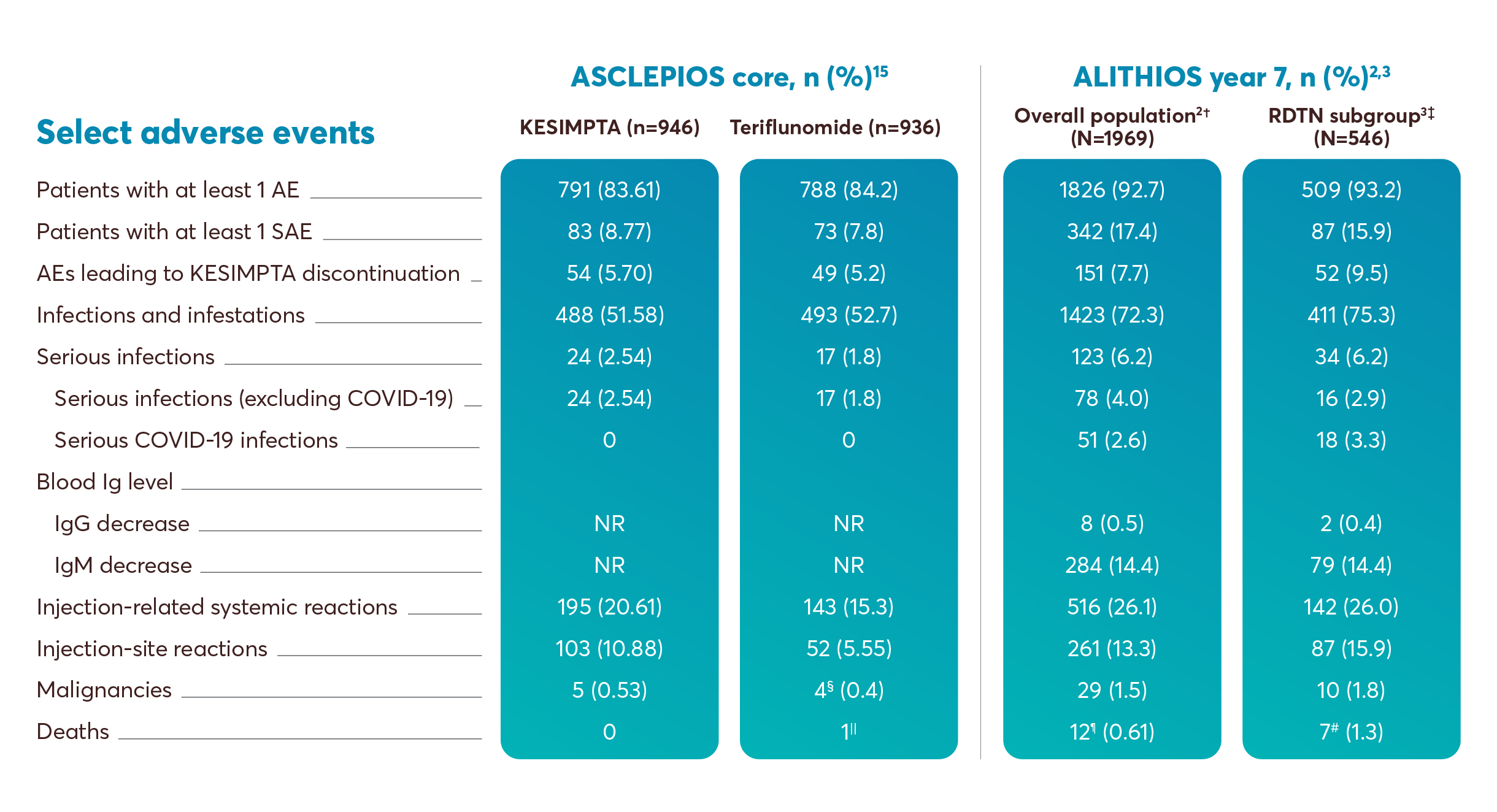
No New Safety Signals Were Identified in the ALITHIOS Extension Study at 7 Years2*
Expanding upon the established safety profile of KESIMPTA in the ASCLEPIOS I and II clinical trials, there were no new safety signals identified after 7 years in the ALITHIOS trial.*
No conclusions of statistical or clinical outcomes can be drawn.
Mean IgG levels remained >LLN (5.65 g/L) in 96.8% of participants at all assessments. Mean IgM levels decreased but remained >LLN (0.4 g/L) and were >LLN at all assessments in 64.5% of participants. The proportion of participants with Ig-related AEs leading to ofatumumab interruption or discontinuation due to low IgG was 0.2%/0.2% and for low IgM was 10.4%/3.6%.2
Mean IgG levels remained >LLN (5.65 g/L) in 97.6% of participants at all assessments. Mean IgM levels decreased but remained >LLN (0.4 g/L) and were >LLN at all assessments in 62.4% of participants. The proportion of participants with Ig-related AEs leading to ofatumumab interruption or discontinuation due to low IgG was 0.0%/0.2% and for low IgM was 9.7%/4.2%.3
AE, adverse event; SAE, serious adverse event; COVID-19, coronavirus disease 2019; Ig, immunoglobulin; IgG, immunoglobulin G; IgM, immunoglobulin M; RDTN, recently diagnosed treatment-naïve; LLN, lower limit of normal.
*Safety signals have been identified through post-marketing studies for anti-CD20s approved for the treatment of multiple sclerosis, including KESIMPTA. Refer to Full Prescribing and Important Safety Information.1
†Included participants receiving ≥1 dose of ofatumumab in ASCLEPIOS I/II, APOLITOS, APLIOS, or the ALITHIOS extension study.2
‡Included RDTN subgroup safety population receiving ≥1 dose of ofatumumab in ASCLEPIOS I/II or ALITHIOS.3
§One case of basal cell carcinoma was not listed as an SAE.15
||Death was due to aortic dissection.15
¶Including the following: Sudden death (n=1), esophageal adenocarcinoma (n=1), completed suicide (n=1), COVID-19/COVID-19 pneumonia (n=1), COVID-19 (n=2), gastric ulcer perforation (n=1), COVID-19 pneumonia (n=1), intestinal metastasis (n=1), COVID-19 pneumonia/pneumothorax (n=1), pneumonia/septic shock (n=1), and injury (n=1).2
#Including the following: Sudden death (n=1), esophageal adenocarcinoma (n=1), completed suicide (n=1), aortic dissection (n=1), COVID-19/COVID-19 pneumonia (n=1), and COVID-19 (n=2).3
Mean IgG and IgM Levels Remained Above the Lower Limit of Normal for Up to 7 Years of Treatment2
Mean IgG levels remained >LLN (5.65 g/L) in 96.8% of participants at all assessments for up to 7 years.2
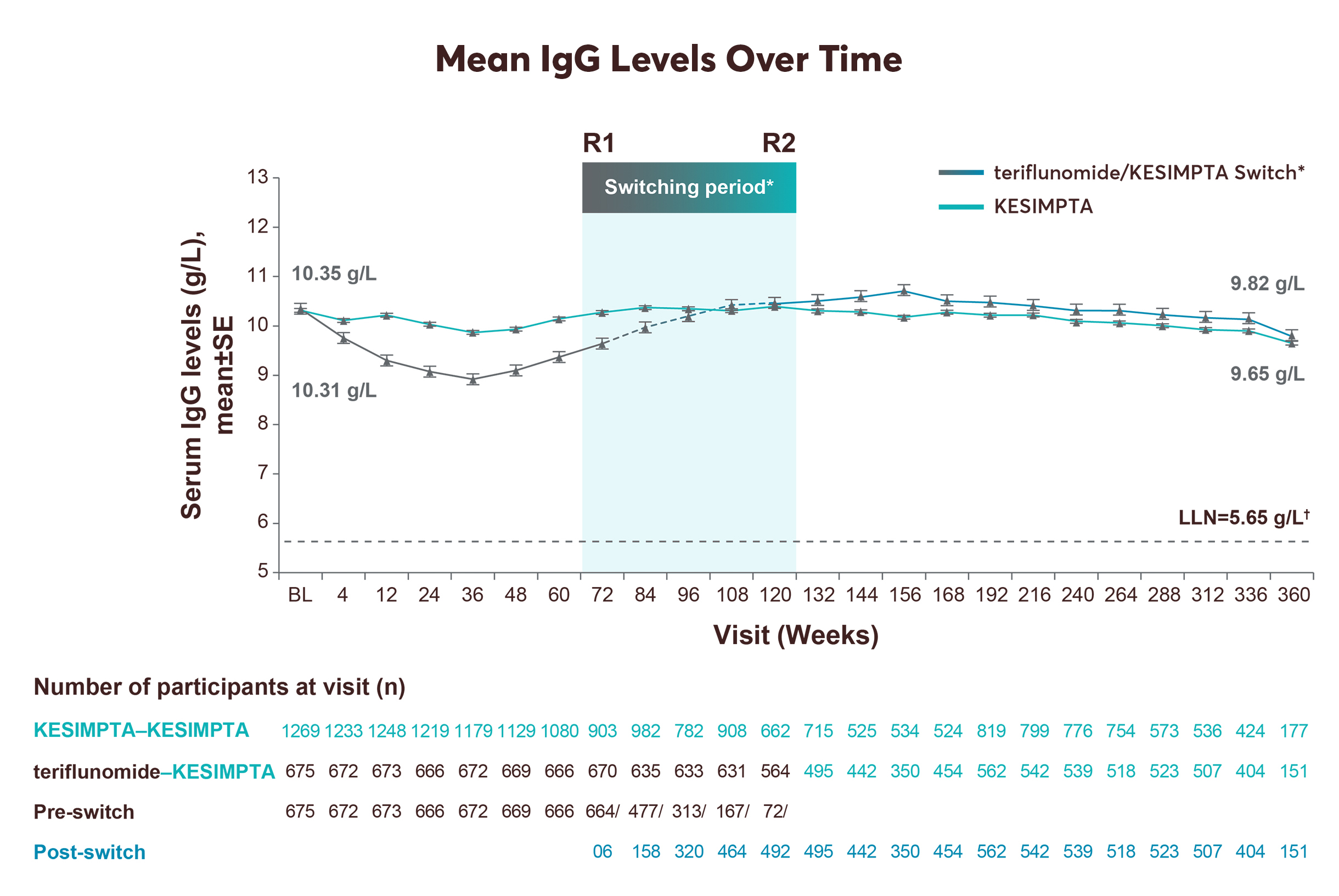
No conclusions of statistical or clinical outcomes can be drawn.
Mean IgM levels remained >LLN (0.4 g/L) in 64.5% of participants at all assessments. In the long-term analysis, mean IgM levels declined but remained above the LLN.2
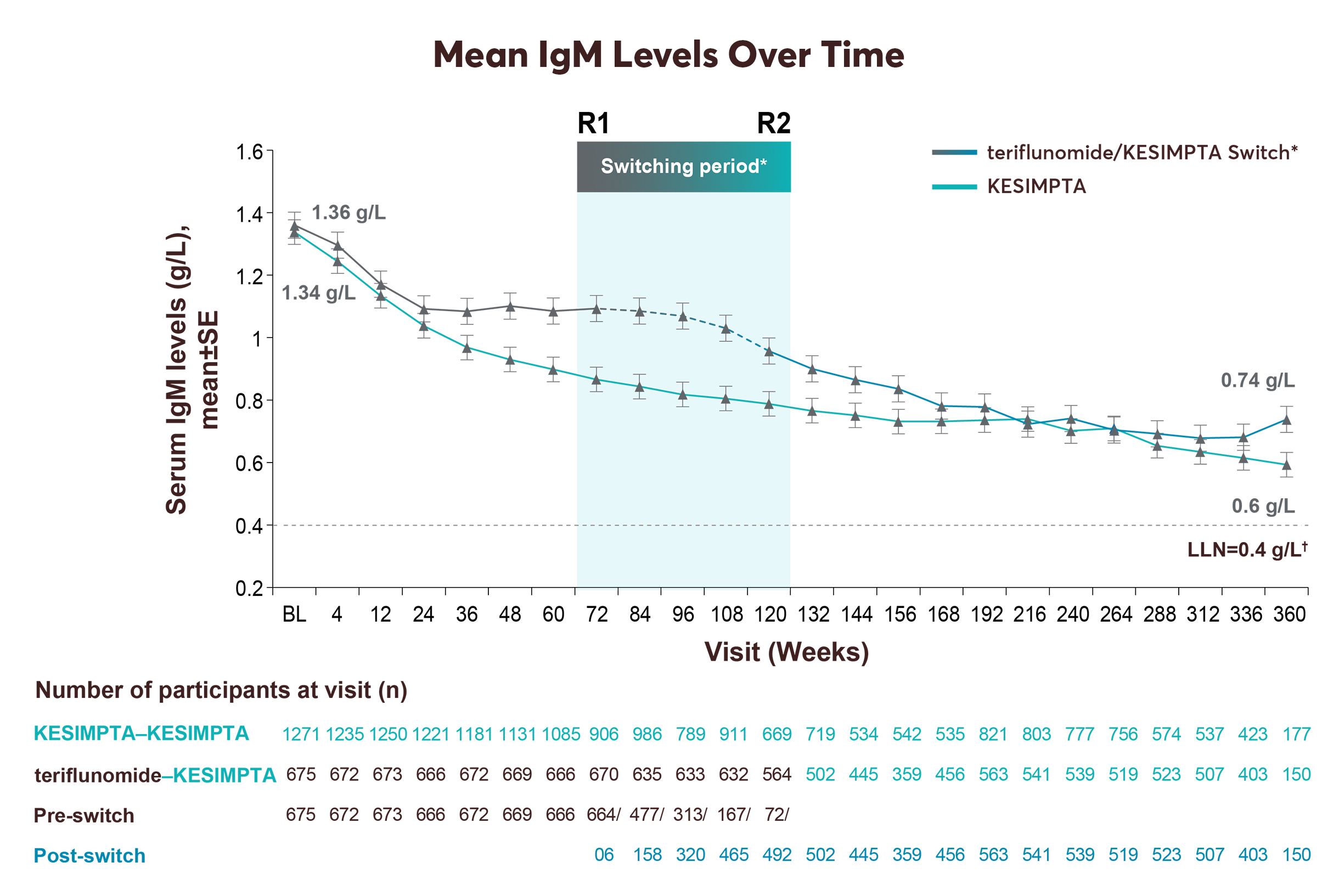
No conclusions of statistical or clinical outcomes can be drawn.
Treatment interruption/discontinuation was reported in 3 (0.2%)/4 (0.2%) participants due to low IgG, and in 204 (10.4%)/71 (3.6%) participants due to low IgM.2
Serious, including life-threatening or fatal, bacterial, fungal, and new or reactivated viral infections have been observed during and following completion of treatment with anti-CD20 B-cell depleting therapies.
*Switching period refers to the participants started on teriflunomide and not applicable to the participants on ofatumumab in the core period. For the teriflunomide/ofatumumab group, data from the first dose of teriflunomide until the last dose of ofatumumab plus 100 days or analysis cut-off date has been used. R1: The first participant with first treatment-emergent assessment in ofatumumab period after switching to ofatumumab (72 weeks); R2: The last participant with last treatment-emergent assessment in teriflunomide period before switching to ofatumumab (120 weeks).2
†For all pooled analyses, a fixed value of LLN (using ALITHIOS study reference) was used: IgG: 5.65 g/L and IgM: 0.4 g/L.2
In clinical practice, I've seen patients' IgG and IgM levels change over time, similar to these results, but it's reassuring to know that the immunoglobulins remained above the LLN with KESIMPTA patients in the study.2
—Amy Perrin Ross, APN, MSN, CNRN, MSCN
IgG, immunoglobulin G; IgM, immunoglobulin M; LLN, lower limit of normal; SE, standard error.
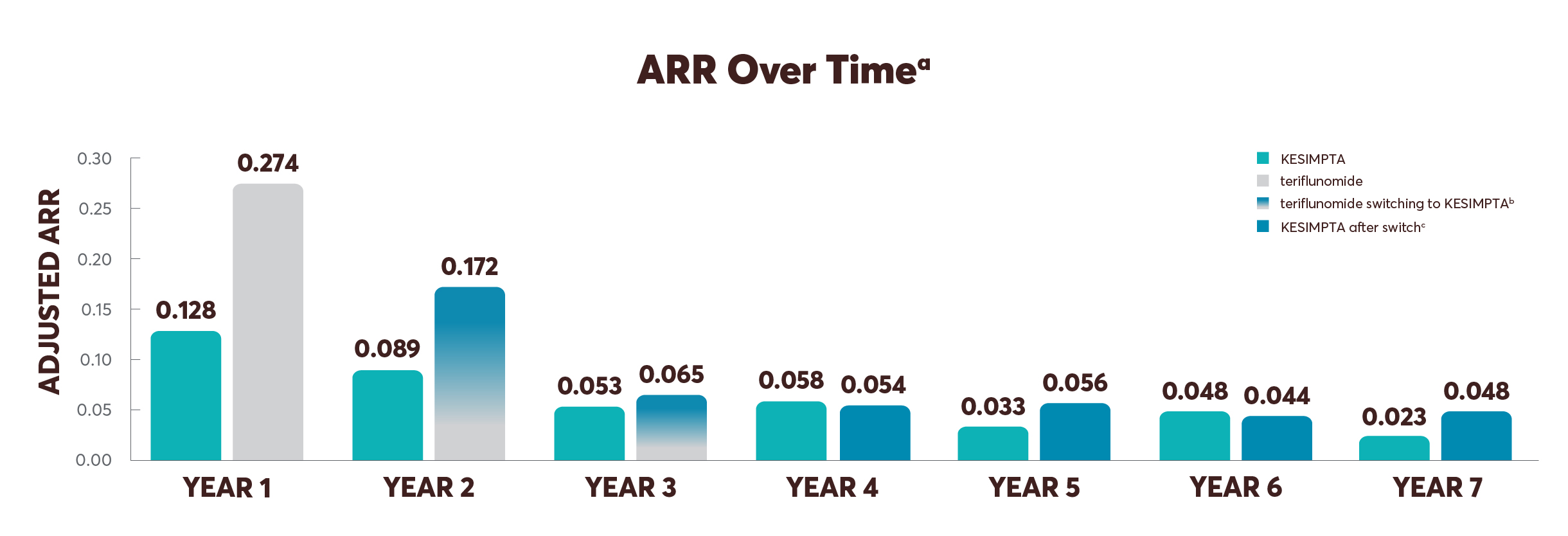
ARR was 0.128 at year 1 and remained below that level, decreasing to an ARR of 0.023 at year 7 with continuous KESIMPTA—the lowest level recorded across all years of the study up to 7 years of the study with continuous KESIMPTA.2
ALITHIOS study design: ALITHIOS is an open-label, umbrella-extension, Phase 3b, single-arm study evaluating long-term (up to 7 years) data. The primary objective is to assess safety and tolerability (N=1969) in patients with RMS who had at least 1 dose of KESIMPTA (20 mg SC) (including dropouts) from the ASCLEPIOS I/II, APLIOS, and APOLITOS trials. APLIOS (N=284) was a Phase 2, 12-week, open-label, parallel-group study. APOLITOS (N=62) is a Phase 2, 24-week, double-blind, placebo-controlled, parallel-group core-part followed by an open-label extension–part for up to 48 weeks study in Japan and Russia. The secondary objective was to assess efficacy (N=1367) in patients with RMS who had at least 1 dose of KESIMPTA (20 mg SC) from the ASCLEPIOS I and II trials who continued or switched to KESIMPTA treatment. Long-term (up to 7 years) analysis (n=465) was conducted to evaluate efficacy in the recently diagnosed treatment-naïve subgroup treated with KESIMPTA.2,3,9,11,13,14
Limitations: This analysis represents chance findings. The open-label extension study was not blinded, not controlled, and included inherent self-selection bias for remaining in the trial.
No conclusions of statistical or clinical significance can be drawn.
ARR, annualized relapse rate; CDP, confirmed disability progression; EDSS, Expanded Disability Status Scale; Gd+, gadolinium-enhancing; MRI, magnetic resonance imaging; NEDA, no evidence of disease activity; RMS, relapsing multiple sclerosis; SC, subcutaneous.
The reduced risk of relapses is a story worth telling. Personally, I prefer to start KESIMPTA as soon as possible for the right patients.1,2
—Stephen L. Hauser, MD
aBased on confirmed relapses (those accompanied by a clinically relevant change in the EDSS). ARR is obtained from a negative binomial model on treatment, period, region, number of relapses in previous year, baseline EDSS, baseline number of Gd+ lesions, age at baseline, and a treatment-by-period interaction. Log-transformed exposure time (in years) per period is included as an offset variable to annualize the relapse rate in each period. bTeriflunomide-KESIMPTA switch: participants transitioning from teriflunomide to KESIMPTA; due to event-driven core study design (flexible duration), participants transitioned at various exposure time points, ie, the switch from teriflunomide to KESIMPTA started from year 2 and was completed by year 3. cKESIMPTA after switch: teriflunomide participants now on KESIMPTA.
Risk Reduction in MRI Activity Shown for Up to 7 Years with KESIMPTA2,12
A risk reduction of Gd+ T1 lesion activity was observed from years 1 to 7 in the continuous KESIMPTA group and from years 3 to 7 in the group of patients who switched from teriflunomide to KESIMPTA.2,16
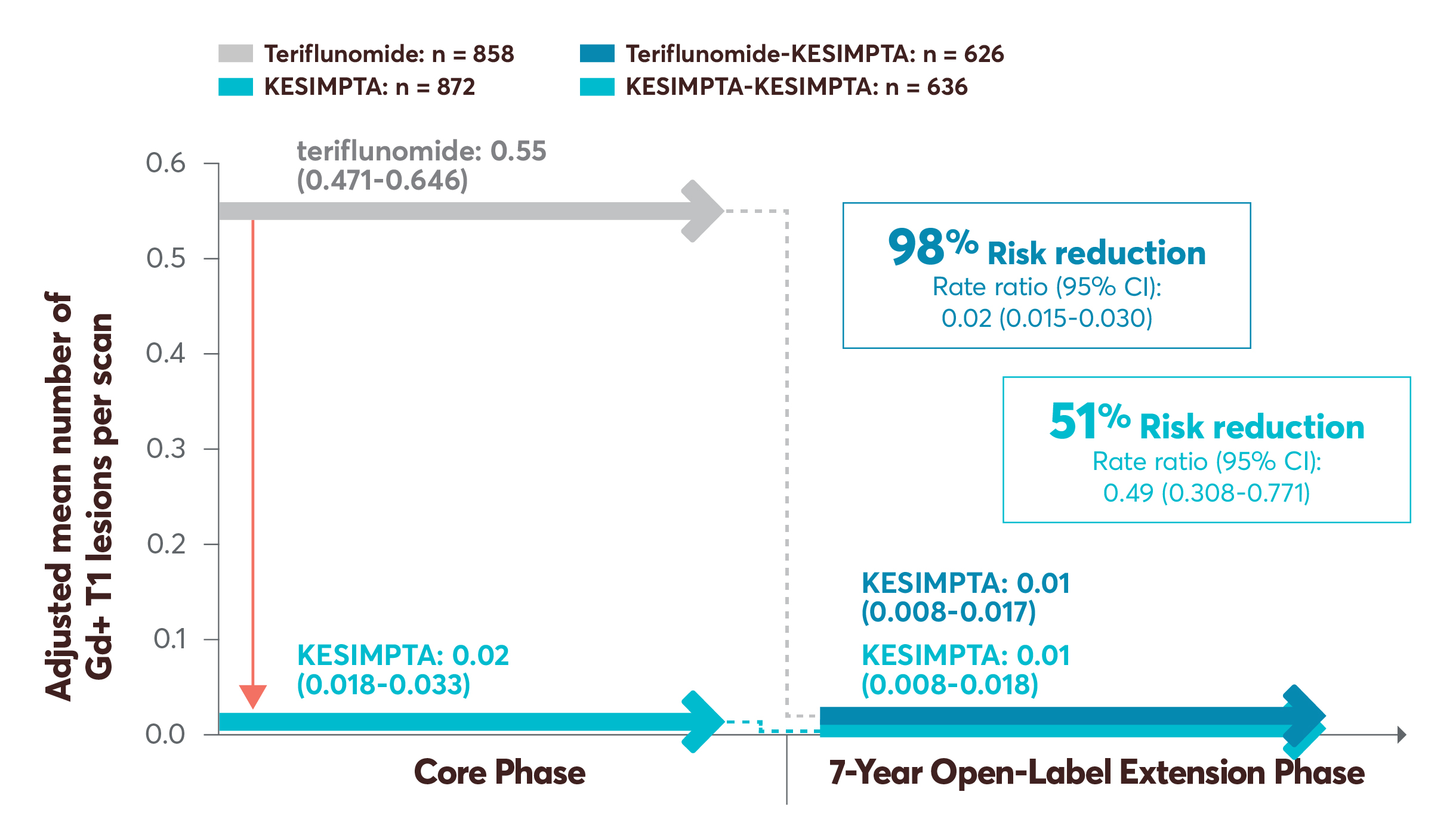
A risk reduction of NE T2 lesion activity was observed by year 2 in the continuous group and was also observed in the group of patients who switched to KESIMPTA from teriflunomide by year 4 and was demonstrated in both groups through year 7.2,16
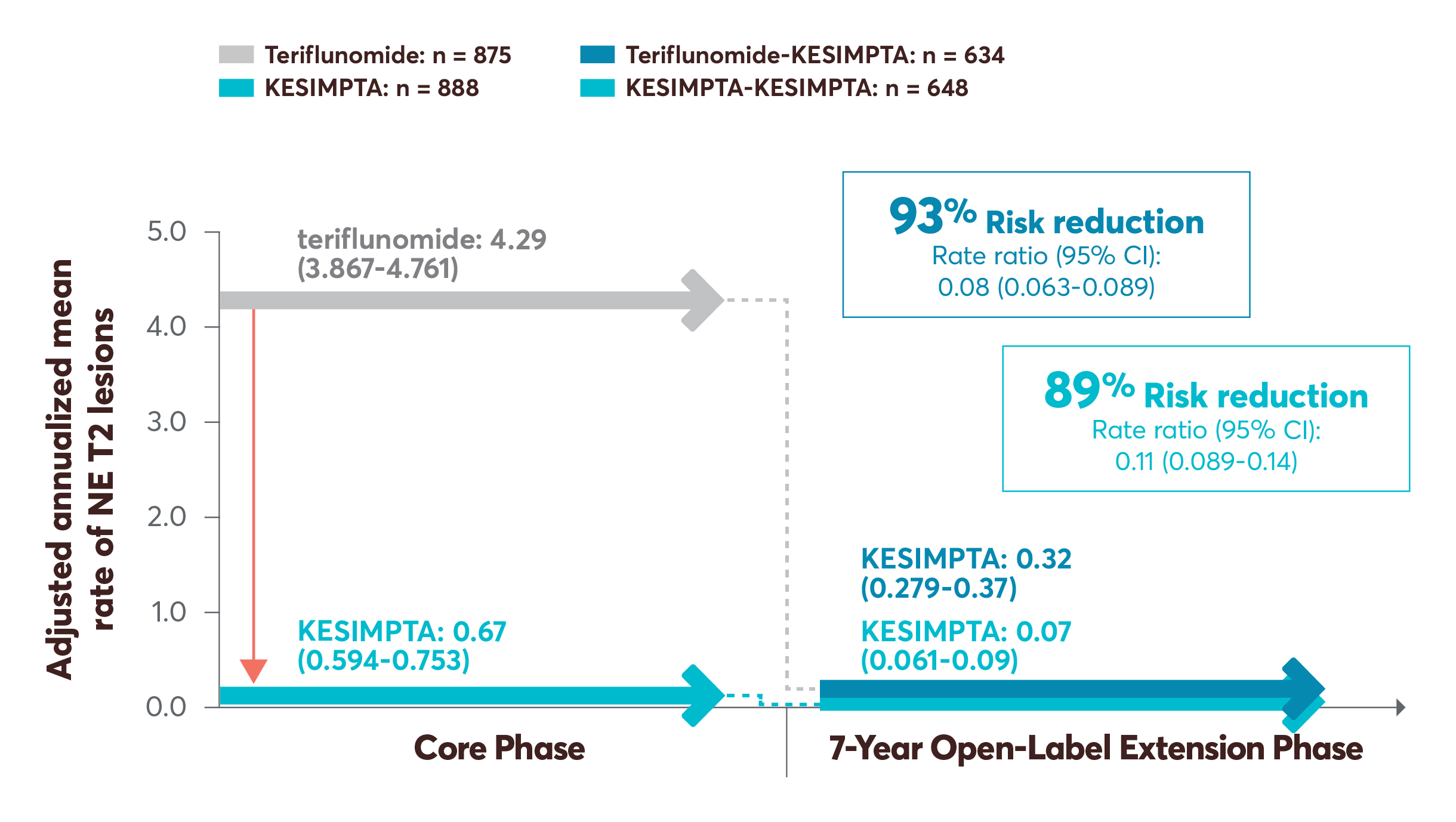
No conclusions of statistical or clinical significance can be drawn.
CI, confidence interval; Gd+, gadolinium-enhancing; MRI, magnetic resonance imaging; NE, new or enlarging.
Nearly 8 out of 10 Patients on Continuous KESIMPTA Were Free From 6mCDP in the Overall Population17
At 7 years, a higher percentage of participants who stayed on KESIMPTA vs those who switched from teriflunomide to KESIMPTA remained free from 6mCDP (77.31% vs 73.84%, respectively).17
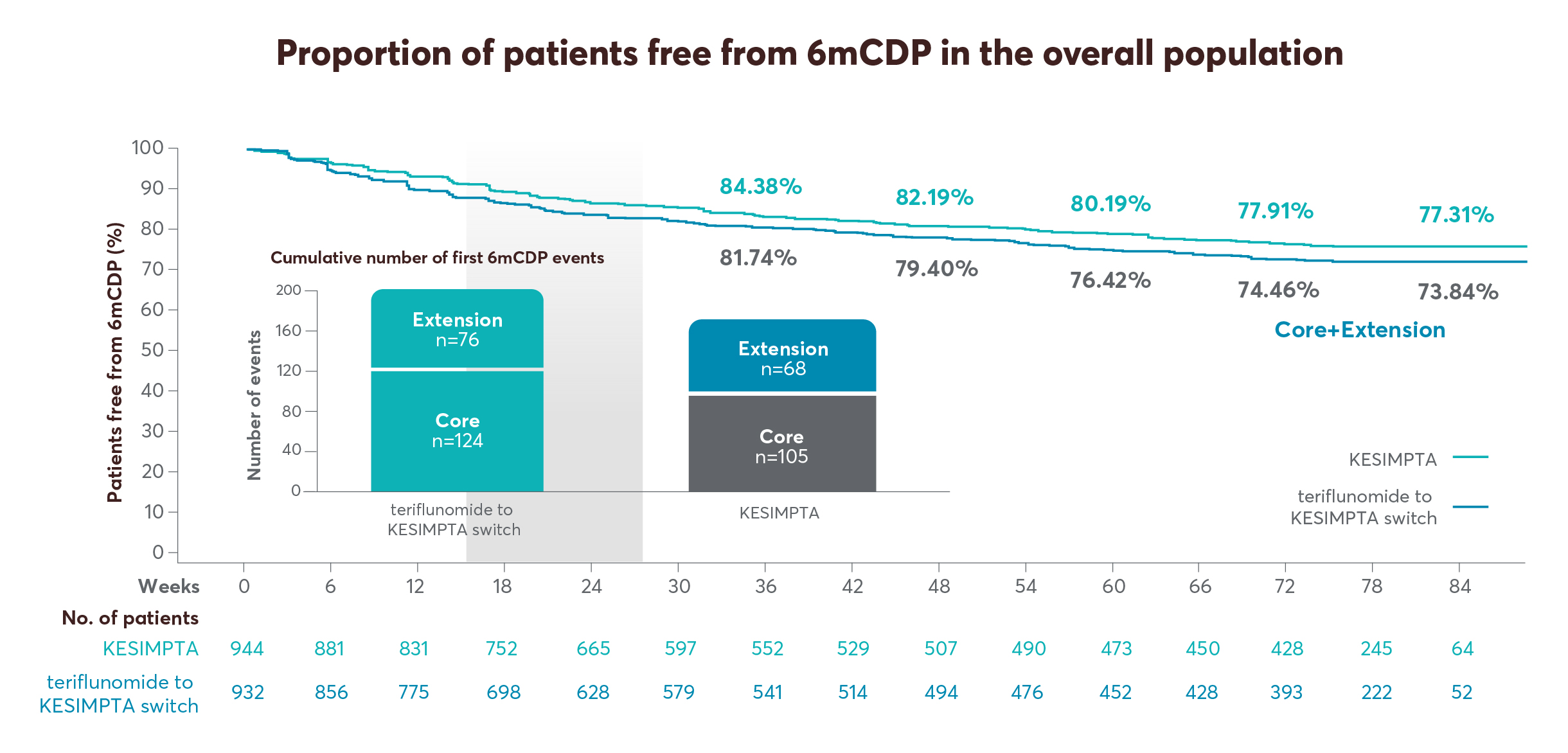
No conclusions of statistical or clinical significance can be drawn.
CDP was defined as an increase from baseline in the EDSS score (≥1.5, ≥1, or ≥0.5 points for patients with a baseline EDSS score of 0, 1-5, or ≥5.5, respectively) sustained for ≥3 (3mCDP) or ≥6 (6mCDP) months.
3mCDP, 3-month confirmed disability progression; 6mCDP, 6-month confirmed disability progression; CDP, confirmed disability progression; EDSS, Expanded Disability Status Scale; OMB, ofatumumab; TER, teriflunomide
The reality is, in a progressive disease like MS, patients can accumulate disability over time. This chart helps visualize the disability gap between patients who start KESIMPTA early and those who switch at a later time.1,17
—Stephen L. Hauser, MD
At Year 7, 95% of Patients Who Started On and Remained on KESIMPTA Achieved NEDA-32
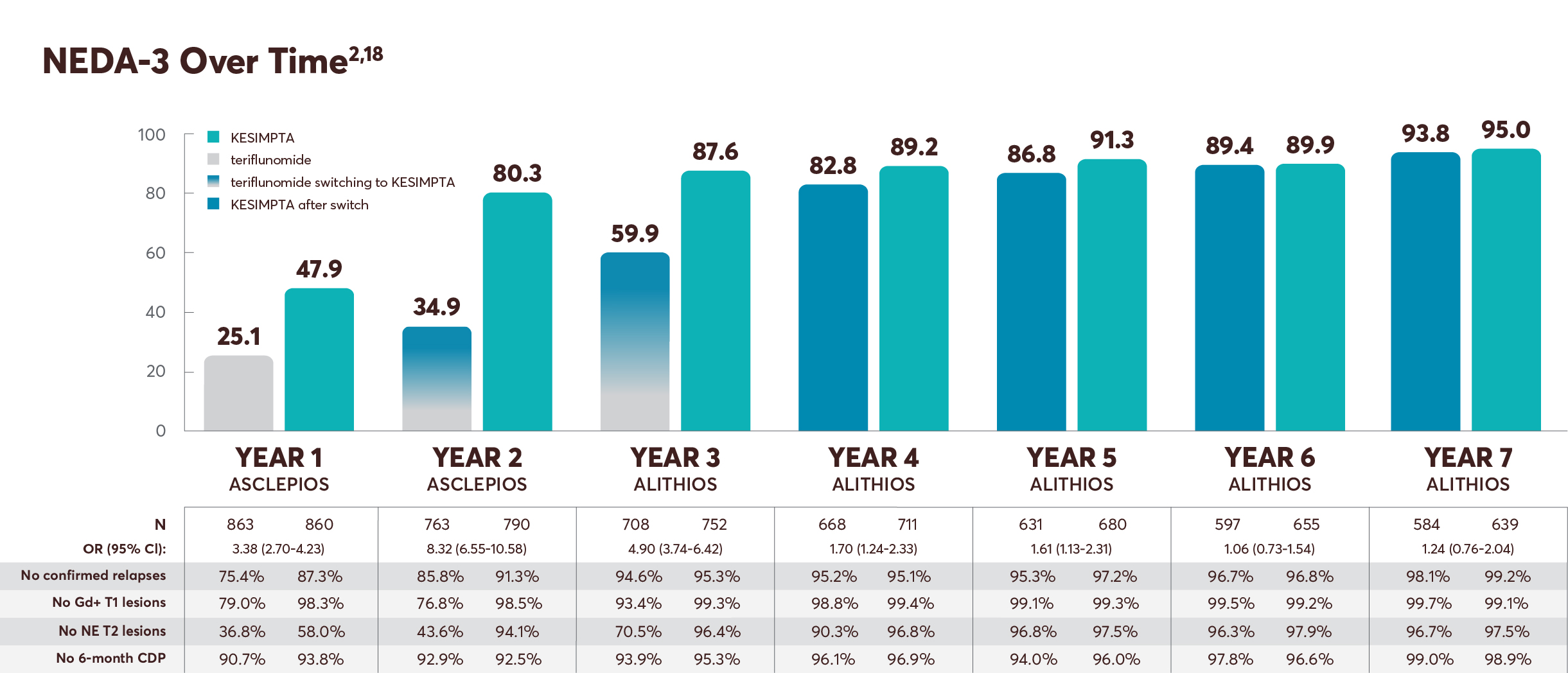
Rebaselining for year 2 (months 12-24) was conducted at month 12 to adjust for impact of disease activity prior to treatment initiation (T2 lesions) and continuing through the first year of treatment. This rebaselining allows for the accurate measurement of the disease activity as measured in year 2.19,20
Limitations: This analysis considers patients without evidence of disease activity (which may also include patients with partially missing information) as NEDA-3. A sensitivity analysis was conducted for the population of patients who completed the full 24 months of treatment.19
NEDA-3 post hoc analysis design: All patients from the pivotal trial, full analysis set population (all randomized patients with assigned treatments), and who received KESIMPTA in the ALITHIOS extension study (data cutoff: September 25, 2024) were included in the intent-to-treat population, but patients who discontinued the study drug prematurely for reasons other than “lack of efficacy” or “death” and had NEDA-3 before early discontinuations were excluded. The outcomes presented here are the proportion of study patients within a treatment group who met the NEDA-3 criteria vs those who did not. The proportion of patients meeting NEDA-3 criteria was analyzed cross-sectionally in 1-year time intervals across 7 years. Within the prespecified time period, patients who achieved NEDA-3 experienced no 6mCDP, no confirmed relapse, no Gd+ T1 lesions, no NE T2 lesions, and no discontinuation from the study drug due to either lack of efficacy or death.2,15,19
No conclusions of clinical outcomes can be drawn.
6mCDP, 6-month confirmed disability progression; CI, confidence interval; Gd+, gadolinium-enhancing; MS, multiple sclerosis; NE, new or enlarging; NEDA, no evidence of disease activity; OR, odds ratio.
What has Dr Hauser seen and considered in his practice with KESIMPTA?
When a patient of mine was diagnosed with RMS, they urgently needed treatment that could offer flexible administration to fit their hectic schedule while they attended medical school.
Once KESIMPTA became available, we reviewed the options and agreed that a self-administered, at-home, once-monthly treatment schedule would fit their lifestyle. Over 5 years later, they have remained on KESIMPTA, and their results aligned with the long-term data.
They eventually graduated medical school and are a practicing physician today. For me, managing RMS means focusing on efficacy and safety while also supporting patients in fitting their RMS treatment into their lives.
—Stephen L. Hauser, MD
RMS, relapsing multiple sclerosis.
Continued Insights and Outcomes With KESIMPTA
Powerful efficacy* and an established safety and tolerability profile1,8,15
Provided patients with at-home self-administration, which can help give them a sense of control and independence over their RMS treatment1
The long-term data offer the opportunity for discussions of KESIMPTA extension data.2 I have had patients on KESIMPTA since the beginning. Each time I get to see a new data release on KESIMPTA, I know that I have something extra I can add to patient discussions at the next touch point.
—Amy Perrin Ross, APN, MSN, CNRN, MSCN
ARR, annualized relapse rate; CDP, confirmed disability progression; Gd+, gadolinium-enhancing; MRI, magnetic resonance imaging; NE, new or enlarging; RMS, relapsing multiple sclerosis.
*As evidenced by reduction in ARR, MRI (Gd+ T1 and T2 lesions), and 3- and 6-month CDP vs teriflunomide. Primary end point: ARR 51% (0.11 vs 0.22), 58% (0.10 vs 0.25). Secondary end points: reduction of number of Gd+ T1 lesions per scan, 98% (0.01 vs 0.46), 94% (0.03 vs 0.52); reduction of annualized rate of NE T2 lesions, 82% (0.72 vs 4.00), 85% (0.64 vs 4.16); 3-month CDP, risk reduction 34% (10.9% vs 15.0%); 6-month CDP, risk reduction 32% (8.1% vs 12.0%).1,8
References:
1. Kesimpta. Prescribing information. Novartis Pharmaceuticals Corp.
2. Hauser SL, Bar-Or A, Cross AH, et al. Continuous ofatumumab treatment for up to 7 years shows a favourable safety and efficacy profile in people with relapsing multiple sclerosis. P804. Presented at: 41st Congress of the European Committee for Treatment and Research in Multiple Sclerosis; September 24-26, 2025; Barcelona, Spain.
3. Bittner S, Hauser SL, Pardo G, et al. Continuous ofatumumab treatment up to 7 years shows a consistent safety and efficacy profile in recently diagnosed treatment-naive people living with relapsing multiple sclerosis. P805. Presented at: 41st Congress of the European Committee for Treatment and Research in Multiple Sclerosis; September 24-26, 2025; Barcelona, Spain.
4. Gorritz M, Chen C-C, Tuly R, et al. Real-world persistence of ofatumumab versus oral disease modifying therapies (DMTs) in patients with multiple sclerosis (MS). LB15. Presented at: 2023 CMSC Annual Meeting; May 31-June 3, 2023; Aurora, CO.
5. Gorritz M, Chen C-C, Tuly R, et al. Real-world persistence and adherence to ofatumumab versus other self-injectable disease modifying therapies (DMTs) in patients with multiple sclerosis (MS). DMT25. Presented at: CMSC Annual Meeting 2023; May 31-June 3, 2023; Aurora, CO.
6. Tai M-H, Brown B, Taiji R, Leung L, Vekeman F, Gadkari A. Persistence and adherence to ofatumumab vs ocrelizumab in commercially insured patients with multiple sclerosis: a real-world retrospective study. P393. Presented at: Americas Committee for Treatment and Research in Multiple Sclerosis Annual Meeting; February 27-March 1, 2025; West Palm Beach, FL.
7. Ross AP, Nicholas J, Tai M-H, et al. Real-world satisfaction and experience with injection and autoinjector device for ofatumumab indicated for multiple sclerosis. LB09. Presented at: Consortium of Multiple Sclerosis Centers Annual Meeting; May 31-June 3, 2023; Aurora, CO.
8. Hauser SL, Bar-Or A, Cohen JA, et al; ASCLEPIOS I and ASCLEPIOS II Trial Groups. Ofatumumab versus teriflunomide in multiple sclerosis. N Engl J Med. 2020;383(6):546-557. doi:10.1056/NEJMoa1917246
9. Hauser SL, Cross AH, Winthrop K, et al. Safety experience with continued exposure to ofatumumab in patients with relapsing forms of multiple sclerosis for up to 3.5 years. Mult Scler. 2022;28(10):1576-1590. doi:10.1177/13524585221079731
10. Hauser SL, Kappos L, Bar-Or A, et al. The development of ofatumumab, a fully human anti-CD20 monoclonal antibody for practical use in relapsing multiple sclerosis treatment. Neurol Ther. 2023;12(5):1491-1515. doi:10.1007/s40120-023-00518-0
11. Long-term safety, tolerability and effectiveness study of ofatumumab in patients with relapsing MS (ALITHIOS). ClinicalTrials.gov identifier: NCT03650114. Updated April 24, 2025. Accessed May 1, 2025. https://clinicaltrials.gov/study/NCT03650114
12. Data on file. Gd+ T1 lesions pooled data at year 7. Novartis Pharmaceuticals Corp; East Hanover, NJ. February 2025.
13. Bar-Or A, Wiendl H, Montalban X, et al. Rapid and sustained B-cell depletion with subcutaneous ofatumumab in relapsing multiple sclerosis: APLIOS, a randomized phase-2 study. Mult Scler. 2022;28(6):910-924.
14. Kira JI, Nakahara J, Sazonov DV, et al. Effect of ofatumumab versus placebo in relapsing multiple sclerosis patients from Japan and Russia: phase 2 APOLITOS study. Mult Scler. 2022;28(8):1229-1238.
15. Wiendl H, Hauser SL, Nicholas J, et al. Longer-term safety and efficacy of ofatumumab in people with relapsing multiple sclerosis for up to 6 years. P9.010. Presented at: 76th American Academy of Neurology Annual Meeting; April 13-18, 2024; Denver, CO.
16. Data on file. NE T2 lesions pooled data at year 7. Novartis Pharmaceuticals Corp; East Hanover, NJ. February 2025.
17. Pardo G, Bar-Or A, Montalban X, et al. Continuous ofatumumab treatment up to 7 years shows a consistent safety profile and delays disability progression in people with relapsing multiple sclerosis. P7.016. Presented at: American Academy of Neurology Meeting; April 5-9, 2025; San Diego, CA.
18. Data on file. Summary of NEDA-3 components per year. Novartis Pharmaceuticals Corp; East Hanover, NJ. September 2025.
19. Data on file. OMB157G (ofatumumab). Statistical overview. Novartis Pharmaceuticals Corp; East Hanover, NJ. December 2019.
20. Giovannoni G, Turner B, Gnanapavan S, Offiah C, Schmierer K, Marta M. Is it time to target no evident disease activity (NEDA) in multiple sclerosis? Mult Scler Relat Disord. 2015;4(4):329-333. doi:10.1016/j.msard.2015.04.006
KESIMPTA Important Safety Information | Click here for full Prescribing Information, including Medication Guide.
KESIMPTA Important Safety Information | Click here for full Prescribing Information, including Medication Guide. ▾
IMPORTANT SAFETY INFORMATION
Contraindications: KESIMPTA is contraindicated in patients with active hepatitis B virus (HBV) infection, or history of hypersensitivity to ofatumumab, or life-threatening injection-related reaction to KESIMPTA. Hypersensitivity reactions have included anaphylaxis and angioedema.
WARNINGS AND PRECAUTIONS
Infections: Serious, including life-threatening or fatal, bacterial, fungal, and new or reactivated viral infections have been observed during and following completion of treatment with anti-CD20 B-cell depleting therapies.
INDICATION
KESIMPTA is indicated for the treatment of relapsing forms of multiple sclerosis (MS), to include clinically isolated syndrome, relapsing-remitting disease, and active secondary progressive disease, in adults.
Indication
KESIMPTA is indicated for the treatment of relapsing forms of multiple sclerosis (MS), to include clinically isolated syndrome, relapsing-remitting disease, and active secondary progressive disease, in adults.
Important Safety Information
Contraindications: KESIMPTA is contraindicated in patients with active hepatitis B virus (HBV) infection, or history of hypersensitivity to ofatumumab, or life-threatening injection-related reaction to KESIMPTA. Hypersensitivity reactions have included anaphylaxis and angioedema.
Warnings and Precautions
Infections: Serious, including life-threatening or fatal, bacterial, fungal, and new or reactivated viral infections have been observed during and following completion of treatment with anti-CD20 B-cell depleting therapies. The overall rate of infections and serious infections in KESIMPTA-treated patients was similar to teriflunomide-treated patients (51.6% vs 52.7%, and 2.5% vs 1.8%, respectively). The most common infections reported by KESIMPTA-treated patients in relapsing MS (RMS) trials included upper respiratory tract infection (39%) and urinary tract infection (10%). Delay KESIMPTA administration in patients with an active infection until resolved.
Consider the potential increased immunosuppressive effects when initiating KESIMPTA after an immunosuppressive therapy or initiating an immunosuppressive therapy after KESIMPTA.
Hepatitis B Virus: Reactivation: No reports of HBV reactivation in patients with MS treated with KESIMPTA. However, HBV reactivation, in some cases resulting in fulminant hepatitis, hepatic failure, and death, has occurred in patients treated with ofatumumab at higher intravenous doses for chronic lymphocytic leukemia (CLL) than the recommended dose in MS and in patients treated with other anti-CD20 antibodies.
Infection: KESIMPTA is contraindicated in patients with active hepatitis B disease. Fatal infections caused by HBV in patients who have not been previously infected have occurred in patients treated with ofatumumab at higher intravenous doses for CLL than the recommended dose in MS. Perform HBV screening in all patients before initiation of KESIMPTA. Patients who are negative for HBsAg and positive for HB core antibody [HBcAb+] or are carriers of HBV [HBsAg+], should consult liver disease experts before starting and during KESIMPTA treatment.
Progressive Multifocal Leukoencephalopathy: No cases of progressive multifocal leukoencephalopathy (PML) have been reported for KESIMPTA in RMS clinical studies; however, PML resulting in death has occurred in patients being treated with ofatumumab at higher intravenous doses for CLL than the recommended dose in MS. In addition, JC virus infection resulting in PML has also been observed in patients treated with other anti-CD20 antibodies and other MS therapies. If PML is suspected, withhold KESIMPTA and perform an appropriate diagnostic evaluation. If PML is confirmed, KESIMPTA should be discontinued.
Vaccinations: Administer all immunizations according to immunization guidelines: for live or live-attenuated vaccines at least 4 weeks and, whenever possible at least 2 weeks prior to starting KESIMPTA for inactivated vaccines. The safety of immunization with live or live-attenuated vaccines following KESIMPTA therapy has not been studied. Vaccination with live or live-attenuated vaccines is not recommended during treatment and after discontinuation until B-cell repletion.
Vaccination of Infants Born to Mothers Treated with KESIMPTA During Pregnancy. For infants whose mother was treated with KESIMPTA during pregnancy, assess B-cell counts prior to administration of live or live-attenuated vaccines. If the B-cell count has not recovered in the infant, do not administer the vaccine as having depleted B-cells may pose an increased risk in these infants.
Injection-Related Reactions and Hypersensitivity Reactions: KESIMPTA can result in systemic injection-related reactions and hypersensitivity reactions, which may be serious or life-threatening. Injection-related reactions with systemic symptoms occurred most commonly within 24 hours of the first injection, but were also observed with later injections. There were no life-threatening injection reactions in RMS clinical studies.
In the post-marketing setting, additional systemic injection-related reactions and hypersensitivity reactions have been reported, including anaphylaxis, angioedema, pruritus, rash, urticaria, erythema, bronchospasm, throat irritation, oropharyngeal pain, dyspnea, pharyngeal or laryngeal edema, flushing, hypotension, dizziness, nausea, and tachycardia. Most cases were not serious and occurred with the first injection. Symptoms of systemic injection-related reactions may be clinically indistinguishable from acute hypersensitivity reactions.
The first injection of KESIMPTA should be performed under the guidance of an appropriately trained health care professional. If systemic injection-related reactions occur, initiate appropriate therapy. Patients who experience symptoms of systemic injection-related reactions or hypersensitivity reactions with KESIMPTA should be instructed to seek immediate medical attention. If local injection-related reactions occur, symptomatic treatment is recommended.
Reduction in Immunoglobulins: As expected with any B-cell depleting therapy, decreased immunoglobulin levels were observed. Monitor the levels of quantitative serum immunoglobulins during treatment, especially in patients with opportunistic or recurrent infections and after discontinuation of therapy until B-cell repletion. Consider discontinuing KESIMPTA therapy if a patient with low immunoglobulins develops a serious opportunistic infection or recurrent infections, or if prolonged hypogammaglobulinemia requires treatment with intravenous immunoglobulins.
Liver Injury: Clinically significant liver injury, without findings of viral hepatitis, has been reported in the post-marketing setting. Signs of liver injury have occurred weeks to months after administration. Patients treated with KESIMPTA found to have an alanine aminotransferase or aspartate aminotransferase greater than 3 times the upper limit of normal (ULN) with serum total bilirubin greater than 2 times the ULN are potentially at risk for severe drug-induced liver injury.
Obtain liver function tests prior to initiating treatment. Monitor for signs and symptoms of hepatic injury during treatment, including new or worsening fatigue, anorexia, nausea, vomiting, right upper abdominal discomfort, dark urine, or jaundice. If symptoms of liver injury are reported, measure serum aminotransferases, alkaline phosphatase, and bilirubin levels. Discontinue KESIMPTA if liver injury is present and an alternative etiology is not identified.
Fetal Risk: Based on animal data, KESIMPTA can cause fetal harm due to B-cell lymphopenia and reduce antibody response in offspring exposed to KESIMPTA in utero. Transient peripheral B-cell depletion and lymphocytopenia have been reported in infants born to mothers exposed to other anti-CD20 B-cell depleting antibodies during pregnancy. Advise females of reproductive potential to use effective contraception while receiving KESIMPTA and for at least 6 months after the last dose.
Most common adverse reactions: Most common adverse reactions (>10%) are upper respiratory tract infection, headache, injection-related reactions, and local injection-site reactions.
Please see full Prescribing Information, including Medication Guide.
KESIMPTA, the KESIMPTA logo, and SENSOREADY are registered trademarks of Novartis AG.
Use of this website is governed by the Terms of Use and Privacy Policy.
Copyright © 2026 Novartis Pharmaceuticals Corporation. All rights reserved.
3/26
FA-11555170











